Wide complex tachycardia
Wide complex tachycardia
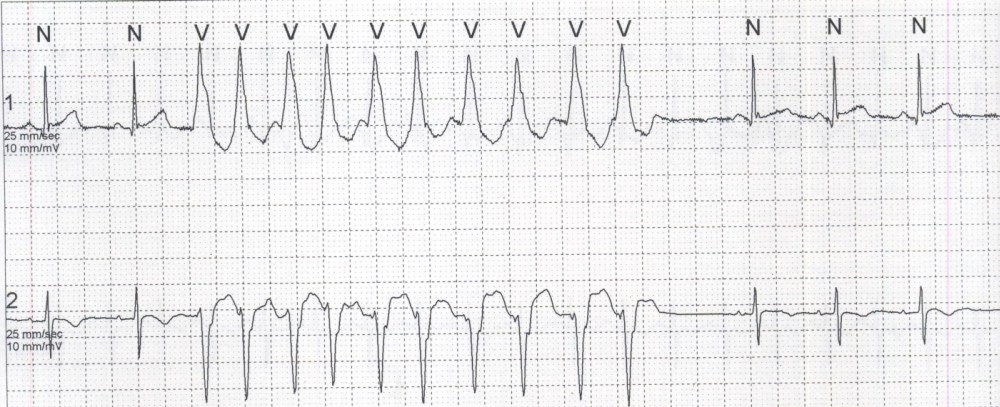
Wide complex tachycardia is otherwise known as wide QRS complex tachycardia or simply wide QRS tachycardia. The general dictum is that wide QRS complex tachycardia is ventricular tachycardia unless proved otherwise. This is because it is the most important form of wide QRS complex tachycardia. Missing a ventricular tachycardia may be more dangerous as well.
Wide QRS Tachycardia
Different types of wide QRS complex tachycardia
Wide QRS complex tachycardia can be either ventricular tachycardia or supraventricular tachycardia with abnormal conduction to the ventricles. SVT usually has a narrow QRS complex while ventricular tachycardia has wide QRS complex. SVT with a pre-existing bundle branch block is another form of wide QRS tachycardia. An antidromic atrioventricular reentrant tachycardia in the presence of prexcitation, WPW syndrome, also has a wide QRS.
When the myocardium is grossly damaged the QRS becomes wide even in a supraventricular rhythm. This can also occur in electrolyte abnormalities like severe hyperkalemia in which the QRS widens and merges with the T wave to produce a ‘sine wave pattern’. Certain drugs and toxins can also produce widening of QRS in a supraventricular rhythm.
Adenosine test for differentiation of wide QRS complex tachycardia
One of the conventional therapeutic tests which is advocated in the differentiation of wide QRS tachycardia is an intravenous bolus of adenosine. Adenosine by producing a transient atrioventricular nodal block, terminates any supraventricular tachycardia which depends on the AV node for maintenance. If it is an atrial tachycardia being conducted through an aberrant pathway or with a pre-existent bundle branch block, conduction ratio will be altered to produce 2:1 or 3:1 conduction.
Since the duration of action of adenosine is less than 30 seconds any adverse effect will be short lived and is unlikely to produce any problem even if it is a ventricular tachycardia. But this test is not as innocuous as it was thought to be earlier. Certain cases of ventricular tachycardia may go into hemodynamic compromise or rarely even cardiac arrest due to ventricular fibrillation can occur with adenosine challenge. Hence a word of caution is required while advocating adenosine as a therapeutic test for wide QRS tachycardia.
Related Posts




About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal